

The rectum is the final part that connects the large intestine to the anus. Its main function is to store stool before it is expelled from the body. The rectum is approximately 12–15 cm long and consists of three layers. The mucosal layer, which contains glands that secrete mucus to facilitate the passage of stool, covers the inner surface of the rectum. The layer called the muscularis propria, which forms the middle layer of the rectal wall, is made up of muscles that enable contraction. The last part of the rectum is a fatty layer. In addition to these three parts, lymph nodes—which are part of the immune system—surround the rectum.
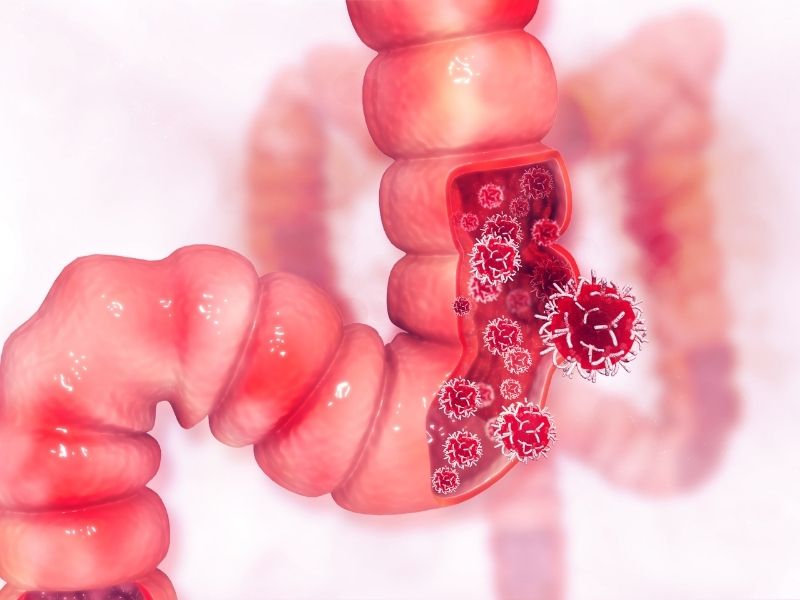
Rectal cancer is a disease in which cancerous (malignant) cells form in the tissues of the rectum. Rectal cancer usually originates from polyps on the inner lining of the rectum. Rectal and colon cancers are often referred to as colorectal cancer.
Although rectal and colon cancers are similar in many ways, their treatments are quite different. The main reason is that the rectum sits in a narrow space and is closely surrounded by other organs and structures.
Symptoms of Rectal Cancer
Symptoms of rectal cancer can appear in different ways. However, many cases are detected during routine screening without any symptoms. Symptoms of rectal cancer include:
- Bleeding from the anus or blood in the stool (most common)
- Mucus in the stool
- Changes in bowel habits such as constipation or diarrhea
- A feeling that the bowels do not empty completely
- Painful bowel movements
- Shortness of breath, dizziness, and rapid heartbeat due to anemia
- Bowel obstruction due to the tumor blocking the passage
- Narrowing of stool caliber
- Unexplained weight loss
Causes of Rectal Cancer
Although the exact cause of rectal cancer is not known, there are many risk factors associated with rectal cancer:
- Older age (>50)
- Alcohol and tobacco use
- A high-fat diet rich in animal products
- History of colorectal cancer or polyps
- Chronic inflammatory diseases of the colon and rectum such as ulcerative colitis and Crohn’s disease
- Genetic syndromes such as hereditary nonpolyposis colorectal cancer (Lynch syndrome) and familial adenomatous polyposis (FAP)
- Sedentary lifestyle and obesity
- Receiving radiotherapy, especially to the abdominal area, for cancer treatment
- Diabetes
- Colon and rectal cancer in first-degree relatives
Diagnosis of Rectal Cancer
Routine screening programs are necessary to diagnose rectal cancer early. In people without risk factors, starting routine screening at age 50 is very important for early detection. In individuals with risk factors, screening should begin earlier. Rectal cancer is often diagnosed during evaluations performed after rectal bleeding or iron deficiency is detected. The following tests may be used in the diagnosis of rectal cancer:
- Rectal examination: A digital (finger) rectal exam performed to feel cancer in the rectal wall. If the tumor is far from the anus, rectal cancer may not be detected with this exam. If an abnormality is found, an endoscopy is performed for further evaluation.
- Colonoscopy & rectoscopy: Using a lighted camera inserted through the anus, the rectum (rectoscopy) or the entire large intestine (colonoscopy) can be examined. This allows direct visualization of the inner surfaces of the rectum and colon. Tissue samples (biopsy) can be taken from suspicious areas, and polyps that can be removed endoscopically may be removed during the procedure.

Staging in Rectal Cancer
After a rectal cancer diagnosis is made, it is necessary to determine the extent (stage) of the cancer. The stage of your cancer helps guide survival expectations and treatment options. Staging tests include:
Complete blood count (CBC): This test reports the number of different cell types in the blood. A low red blood cell count indicates anemia, while elevated white blood cells may suggest a possible infection/inflammation.
Biochemical blood tests: By measuring levels of different chemicals in the blood, organ functions (such as the liver and kidneys) are assessed.
Carcinoembryonic antigen (CEA): Cancers may produce substances called tumor markers that can be detected in the blood. One such marker, CEA, may be higher than normal in people with colorectal cancer. The CEA test is useful for monitoring response to treatment.
Chest CT scan: This imaging test helps determine whether rectal cancer has spread to other organs such as the liver and lungs.
Pelvic MRI: MRI shows in detail how the tumor in the rectum relates to surrounding muscles, organs, and other tissues. It can also show lymph nodes near the rectum and different tissue layers of the rectal wall.
Endoscopic ultrasound (EUS): An advanced test used to evaluate how far the rectal tumor has progressed within the rectal wall and its relationship with surrounding tissues.
Treatment of Rectal Cancer
Treatment planning for rectal cancer depends on the stage and grade of the cancer, the tumor’s location and size within the rectum, and the patient’s age and general health. The primary treatment for rectal cancer is surgery. If complete removal of the tumor is not expected or if the patient’s overall condition cannot tolerate major surgery, drug therapy (chemotherapy) and radiation therapy (radiotherapy) may be used to shrink the tumor and reduce symptoms.
Surgical Treatments
- Endoscopic surgery: In early-stage rectal cancers, the tumor and a margin of healthy rectal wall can be removed using special instruments inserted through the anus. Endoscopic mucosal resection (EMR), endoscopic submucosal dissection (ESD), and transanal local excision are examples. These approaches are suitable for cancers that are non-aggressive, small in size, have not invaded the rectal muscle layer, and have not spread to regional lymph nodes.
- Removal of part or all of the rectum: Larger rectal cancers that are sufficiently far from the anal canal can be treated with an approach that removes part or all of the rectum (low anterior resection). Surrounding tissue and lymph nodes are also removed. Because the anus is preserved, stool leaves the body normally through the anus. However, in some cases, to protect the intestinal connection, a temporary opening of part of the bowel to the abdominal wall (temporary stoma) may be created. This procedure can be performed using an open technique, or laparoscopically (minimally invasive) or robotically in suitable patients.
- Removal of the rectum and anus: In rectal cancers close to the anus, it may not be possible to completely remove the cancer without damaging the muscles that control bowel movements. In this case, the rectum, anus, and part of the colon—along with nearby tissue and regional lymph nodes—may be removed. After an operation called abdominoperineal resection (APR), the anal area is completely closed and part of the intestine is brought out to the abdominal wall to allow stool to exit. This opening is permanent (lifelong). The procedure may be performed openly, or laparoscopically or with robotic surgery in appropriate patients.
Chemotherapy
Chemotherapy involves chemical drugs used to destroy cancer cells. For rectal cancer, chemotherapy is usually given after surgery if the cancer is larger or has spread to lymph nodes. In this way, chemotherapy can kill remaining cancer cells in the body and help reduce the risk of recurrence. In some cases, it may also be given before surgery to shrink the tumor and increase the effectiveness of surgery.
In advanced-stage cancers that cannot be operated on and cancers that have spread throughout the body, it may also be administered together with radiotherapy to reduce symptoms.
Radiotherapy (Radiation Treatment)
Radiation therapy uses powerful energy sources such as X-rays and protons to kill cancer cells. It can be used to shrink a large cancer before surgery so it can be removed more easily.
When surgery is not an option, radiation therapy may be used to relieve symptoms such as pain and bleeding. Sometimes radiation is combined with chemotherapy.
Immunotherapy
Immunotherapy is a drug treatment that uses your immune system to fight cancer. Your disease-fighting immune system may not attack your cancer because cancer cells produce proteins that prevent immune cells from recognizing them as dangerous. Immunotherapy works by interfering with this process. Immunotherapy is generally reserved for advanced rectal cancer.
Survival in Rectal Cancer
Life expectancy in rectal cancer depends on many factors such as the grade and stage of the cancer, carcinoembryonic antigen (CEA) levels, the patient’s general health, the selected treatment method, and the patient’s response to treatment. There is no single definite answer to questions like “How long does a person live with rectal cancer?” and it varies from patient to patient.
According to general statistics worldwide, 5-year survival rates are as follows:
- Stage I: 80–88%
- Stage II: 60–81%
- Stage III: 40–75%
- Stage IV: 8–13%


